The honest verdict up front
This is a legitimate, mechanistically-grounded plausible hypothesis — not speculation, not established fact. It has a real molecular spine and fits the early-onset pattern. What is not established: that any specific chemical causes these cancers, that the microbiome mediates it in people, or that ultra-processed food is more than a marker for a worse overall lifestyle. So: plausibly a contributing cause worth a serious, falsifiable test — and easy to overclaim.
Why it's plausible: a molecular thread to young-adult cancer
There is now a genuine chain linking gut bacteria to early-onset colorectal cancer (CRC):
Colibactin
A DNA-damaging toxin from certain gut E. coli (pks+). Proven to mutate human gut cells in the lab (organoids), leaving two specific "fingerprints" (SBS88/ID18). [Nature 2020]
Early-life imprint
The fingerprint is 3.3× more common in CRC diagnosed under 40 than over 70, is laid down in the first ~10 years of life, and hits APC — the gene that initiates CRC. [Nature 2025]
Ultra-processed diet
A low-fiber diet starves protective butyrate-making bacteria; emulsifiers (in processed food) thin the gut's mucus barrier and let bacteria encroach — shown in mice and a small human trial. [Nature 2015; Gastro 2022]
This is the cleanest answer to "why do healthy young people get cancer?": the leading molecular hypothesis is a childhood microbial/chemical insult that seeds the first mutation decades before a tumor appears — a birth-cohort effect (risk tracks the year you were born, rising for cohorts born after ~1960, exactly when the modern processed-food system arrived).
The suspects (ranked by evidence)
| Agent | Where | Evidence status |
|---|---|---|
| Colibactin / pks+ E. coli | gut bacteria | Established mechanism; ~4–9% of CRC; early-onset enriched |
| Emulsifiers (CMC, polysorbate-80) | processed food | Established in mice + human microbiome RCT; not yet cancer |
| Titanium dioxide (E171) | food coloring | Plausible — EU-banned 2022, still in US food |
| Nitrate → N-nitroso compounds | drinking water | Contested — see the Iowa deep-dive below |
| Artificial sweeteners | food/drink | Microbiome-active (proven), but cancer case weak — possibly net protective |
| PFAS (non-microbiome) | drinking water | IARC Group 1 (PFOA) — but kidney/testicular at HIGH dose |
| Microplastics, antibiotics | food/water | Plausible → speculative; weaker direct evidence |
How would we actually find out? A falsifiable program
The whole challenge is that ultra-processed diet, obesity, low fiber, alcohol, smoking, and poverty all travel together. The program is built to isolate one agent from that bundle by triangulating designs with different weaknesses — and to be provably wrong.
Mechanistic
Organoids + "humanized" mice, at realistic doses (not the 10× doses many scary studies use).
Molecular archaeology
Tumor genomes are a physical archive of past exposure that bias can't fake. Read the colibactin fingerprint and date when it struck.
Human cohorts
Banked stool/serum + microbiome + diet + chemical biomonitoring → does the microbiome mediate the effect?
Causal inference
Mendelian randomization, negative controls (an inert junk-food-tracking additive; a non-gut cancer), mediation.
Natural experiments
EU additive bans vs US; Iowa water-source/nitrate-removal boundaries.
Ecological
Cheapest, weakest (what we have). Generates hypotheses only — never proves causation.
What would falsify it
Rejected if lab effects need 10×+ realistic doses and Iowa early-onset tumors show no colibactin excess and the microbiome mediates ~0% in humans — or if the negative controls "associate" just as strongly (meaning it was lifestyle confounding all along).
Deep dive: nitrate in Iowa's water
Nitrate is the most Iowa-relevant of the water suspects — and the cleanest illustration of why this is hard. Iowa has the worst agricultural-nitrate problem in the country: a county median of 5.7 mg/L vs 1.6 nationally, with 27% of Iowa counties exceeding the 10 mg/L EPA limit (11% nationally).
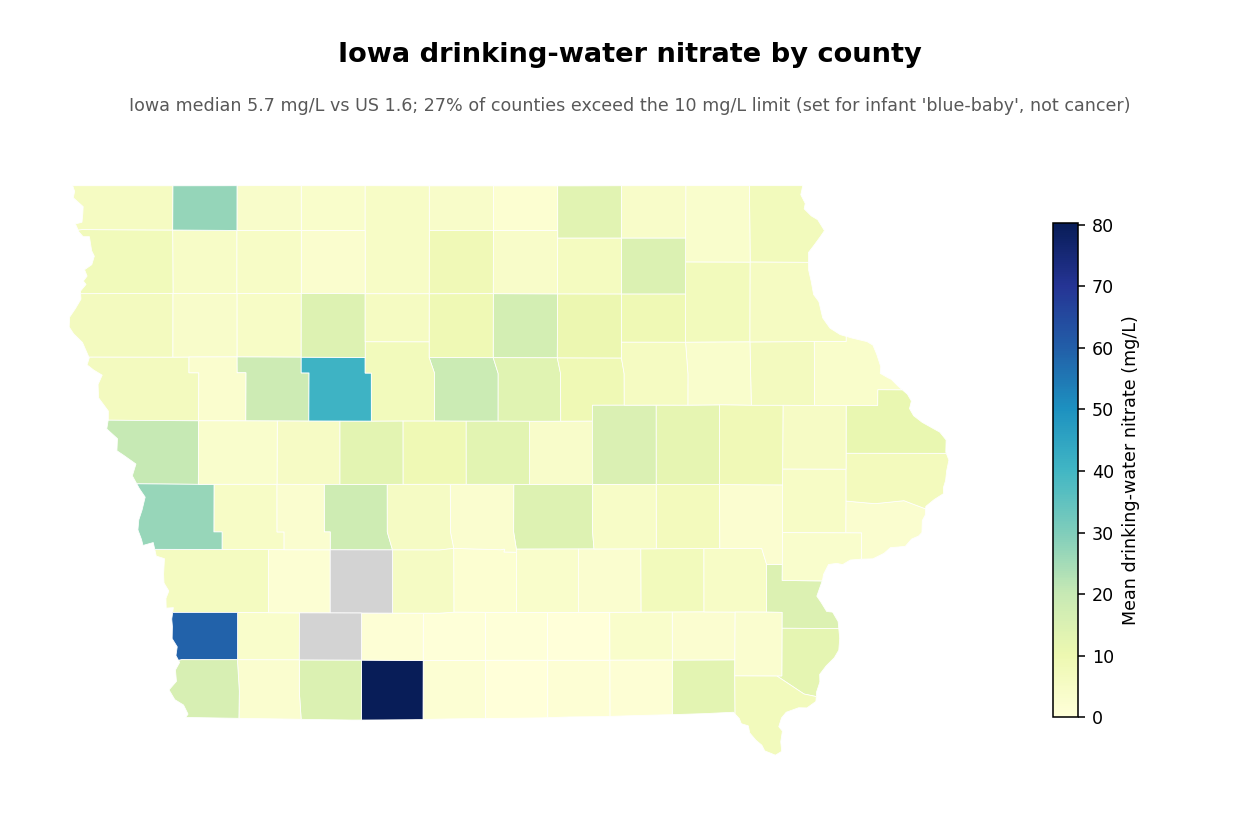
The single most defensible point: Iowa's median is in the "signal band" — below a cancer-blind limit
The 10 mg/L EPA limit was set in 1962 for infant "blue-baby" syndrome — with zero cancer consideration. Yet multiple prospective cohorts find cancer associations below it: colorectal risk rises above ~3.9 mg/L (Schullehner 2018, Denmark, 1.7M people). Iowa's median is 5.7 mg/L — so the typical Iowan sits squarely in the band where the positive studies detect effects, while still being "compliant" with the standard. ~290,000 Iowans on unmonitored private wells are exactly the higher-exposure group where the link is clearest.
The honest split: a real exposure, a contested cancer link
Individual-level cohorts find modest signals: colorectal HR≈1.16 (Schullehner 2018); aggressive prostate HR≈1.22 at >10 mg/L (Spaur 2026, JNCI, Agricultural Health Study); and a real Iowa cohort — the Iowa Women's Health Study — found bladder cancer HR≈1.62 for sustained >5 mg/L (and dietary nitrate was null, pointing to a water-specific effect). But the most-cited meta-analysis (Picetti 2022) is null for colorectal overall (RR 1.05) — though positive for gastric (RR 1.91) and positive again in the private-well subgroup (RR 1.10). A Cochrane re-analysis removing double-counted studies pushed it back up to RR 1.39. The mechanism (nitrate→N-nitroso compounds) is established biochemistry; IARC rates the nitrosation pathway "probably carcinogenic" (2A) — but explicitly not water nitrate as a standalone proven carcinogen.
| Cancer | Strength of water-nitrate link | Best evidence |
|---|---|---|
| Colorectal | Tier 1 (strongest, but contested) | Schullehner 2018 (HR 1.16, effect below the limit) |
| Gastric / stomach | Tier 1 (positive even in the skeptical meta) | Picetti 2022 (RR 1.91) |
| Thyroid | Tier 2 (moderate) | Ward 2018 (HR up to 2.59) |
| Bladder | Tier 2 (Iowa-specific) | Iowa Women's Health Study (HR 1.62; ×3.7 in smokers) |
| Prostate (aggressive) | Tier 2 (new, single cohort) | Spaur 2026 JNCI (HR 1.22) |
| Ovarian, kidney | Tier 3 (weak/unstable) | few studies |
| NHL, pancreas, breast | Tier 4 (null) | — |
What our data shows — and its hard limit
We tested nitrate against the literature's cancer panel across US counties, adjusting for behavior, socioeconomics, and agricultural intensity. The result is an honest null: no cancer rises with county nitrate, and the tiny colorectal signal reverses (to −0.10, p=0.001) once you account for agriculture.
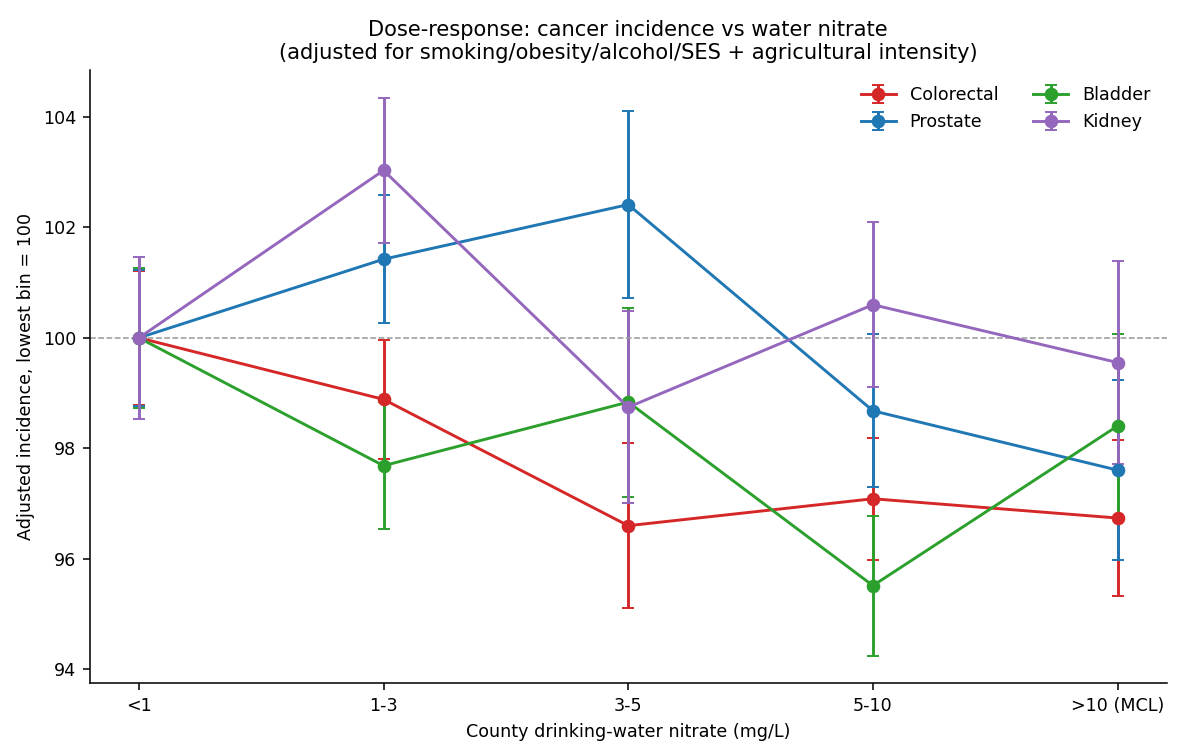
Why this null does NOT clear nitrate
County water-supply nitrate is not individual lifetime ingestion (private wells, bottled water, seasonal spikes, residential moves, decades of cancer latency), and it's a near-perfect proxy for agricultural intensity — which correlates with everything rural. So the ecological design simply cannot test nitrate, exactly as it couldn't test pesticides. The county null and the individual-level cohort signal aren't in conflict; they're answering different questions. You need individual exposure data.
Deep dive: emulsifiers in ultra-processed food
Emulsifiers (carboxymethylcellulose/CMC, polysorbate-80, carrageenan, mono-/diglycerides) are the dietary complement to nitrate's water angle — the additives that make processed food smooth and shelf-stable. They have something nitrate's data can't give: a human feeding trial and a cohort that actually measured intake. But the verdict is, honestly, more skeptical.
Verdict: plausible mechanism, awkward human evidence
Emulsifiers are a plausible contributor to a pro-cancer gut state, but speculative as a cause of human colorectal / early-onset cancer specifically. The chain is strong at its base and weak at its tip. The single most important honest fact: the one large cohort to measure emulsifier intake (NutriNet-Santé, ~92,000 people) found a signal in breast and prostate — and null for colorectal, the exact site the gut mechanism predicts. And CMC/polysorbate-80 (the stars of the mouse studies) showed no human association. Calibrated prior that emulsifiers are a contributory cause of GI cancer at high intake: ~20–30%; that they're a major driver of the early-onset rise: ~5–10%.
The mechanism is serious — and bridges to the colibactin story
In mice, emulsifiers thin the gut's mucus barrier and let bacteria encroach on the lining, shifting the microbiome toward inflammatory species and depleting protective butyrate-makers — and a germ-free transplant experiment proved the harm is microbiome-mediated, not the chemical directly. Here's the elegant connective tissue: colibactin (the early-onset-cancer toxin from the first deep-dive) is only DNA-damaging on direct contact with the gut lining — which intact mucus normally prevents. So emulsifier-thinned mucus could widen the window for colibactin to mutate cells. But this exact combination has never been tested, and the one emulsifier-tumor mouse study found no change in colibactin genes — so the bridge is a clean, falsifiable hypothesis, not a finding.
The human evidence, exactly
| Study | What it found | The honest limit |
|---|---|---|
| FRESH RCT (CMC, 16 people, 11 days) | Microbiome + metabolome perturbed (p=0.001); butyrate down | Bacterial encroachment NOT significant (2/7, p=0.18); no inflammation |
| NutriNet-Santé (~92,000) | Mono-/diglycerides → overall HR 1.15, breast 1.24, prostate 1.46; carrageenan → breast 1.32 | Colorectal null; 160+ comparisons, no correction; UPF not adjusted; self-reported |
The dose problem — with one important exception
The scary mouse doses are ~60–100× the human limit, and the FRESH trial used ~5–100× typical intake — so the population-average alarm is overblown. The exception that matters for your question: the highest real-world exposures are in toddlers and formula-fed infants (up to ~10× adult levels) — i.e., in early life, exactly the birth-cohort window when the early-onset "clock" appears to start. That, plus host-dependent susceptibility, is why "average dose" may be the wrong frame.
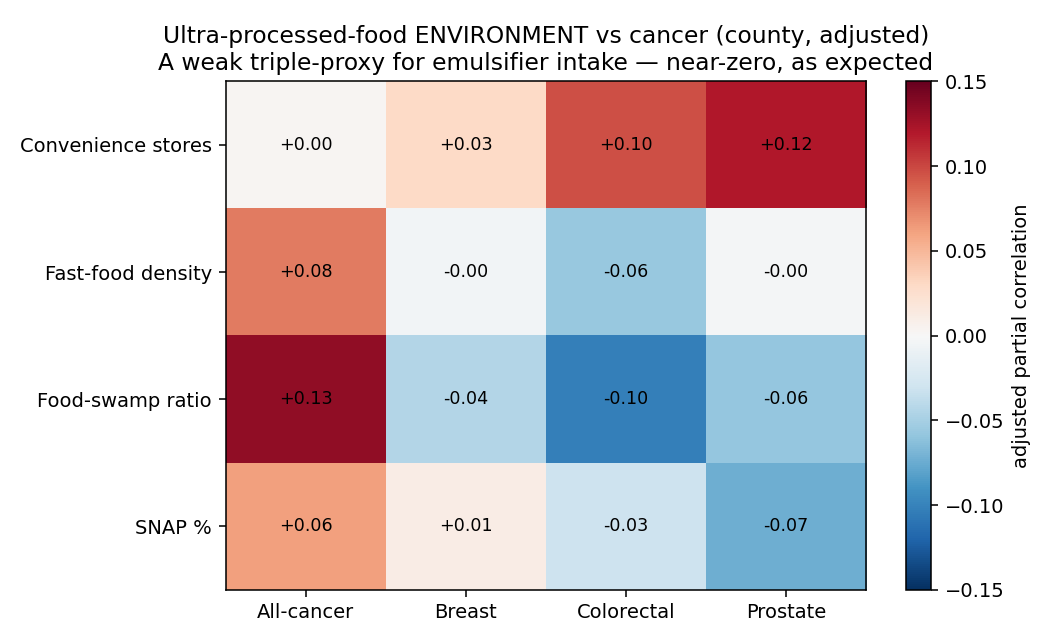
Our data ceiling (and the falsification test that would settle it)
There is no county-level emulsifier data — it's an individual dietary exposure. The only proxy we have is the ultra-processed-food environment, a triple-remove from emulsifier intake. As expected, it's uninformative:
How you'd actually settle it: the inert-additive control
The killer problem is that emulsifier intake is a near-perfect marker for ultra-processed food generally. The decisive design is a "FRESH-2" trial: a 4-arm, 6-week controlled-feeding study including an inert additive that tracks processed food but is microbiome-inert. If the inert control produces the same effect as the emulsifier, the signal was confounding all along — one experiment that can falsify the entire cohort literature. It would also develop the missing piece: a fecal biomarker of emulsifier exposure (CMC isn't absorbed, so there's no blood test — every cohort estimate today is unvalidated self-report). Testable now: UK Biobank (diet + stool sub-cohort + cancer linkage) for a microbiome mediation analysis.
Deep dive: artificial sweeteners
The third suspect — and the one with the strongest microbiome evidence but the weakest cancer case. Sweeteners (sucralose, aspartame, saccharin, acesulfame-K) are where the unbiased process pushes hardest against the hypothesis.
Verdict: microbiome-active, but probably not a cancer cause — and maybe net protective
It is established that sucralose and saccharin causally alter the human gut microbiome at realistic doses (proven by randomized trials where a fecal transplant transferred the effect to germ-free mice). But the proven endpoint is blood-sugar handling, not cancer. The human cancer evidence is weak, inconsistent, and uniquely wrecked by reverse causation. My calibrated priors: ~10–15% that sweeteners are a cause of any cancer at real intake; ~3–5% for the early-onset rise; and — importantly — ~15–25% that they are net protective by displacing sugar.
For your exact question, the data point the other way
In the best early-onset colorectal-cancer cohort (Hur 2021, Gut, ~95,500 women): sugary drinks raised risk (+32% per serving in adolescence), diet drinks showed no association, and swapping a diet drink for a sugary one was tied to 17–36% lower risk. For the young-adult GI cancer we're chasing, the evidence indicts sugar and tentatively favors the sweetener.
The cancer cohort that is positive (NutriNet-Santé: total sweeteners HR 1.13; aspartame 1.15) has an E-value of ~1.5 — obesity alone could manufacture it — and the strongest mechanistic molecule, sucralose, was null in it. Meanwhile a 17-cohort meta-analysis is null (colorectal RR 0.78, decreased) and a 2024 Mendelian-randomization study (which is immune to reverse causation) found no causal link. When only the most-confounded design is positive, the honest read is confounding.
The silver lining (and the colibactin correction)
Unlike emulsifiers, sweeteners have validated urinary biomarkers (acesulfame-K tracks 99% of intake) — so they're genuinely testable: a biomarker-anchored mediation study in a biobank (NHANES already measures them) could settle it. One myth to retire: the popular "Splenda damages your gut DNA via colibactin" claim conflates two different genes — the 2018 finding was about a maltodextrin-binding gene, not the colibactin island — and colibactin imprints in early childhood while sweetener intake peaks later, a temporal mismatch. No evidence links sweeteners to the early-onset colibactin mechanism.
Deep dive: PFAS ("forever chemicals") in Iowa water
The fourth suspect — and a different kind of animal. Unlike the first three, PFAS does not work through the gut microbiome; it's a systemic toxicant. And it carries the strongest cancer credential of the four: in 2023 the WHO's cancer agency classified PFOA as a Group 1 carcinogen (the same evidence tier as tobacco). So this is the one where the hazard is genuinely established — the question is whether Iowa's doses are high enough to matter.
Verdict: a real carcinogen at high exposure; quantitatively small at Iowa tap-water doses
PFOA is an established cause of kidney and testicular cancer at high/occupational exposure (the C8 community near a DuPont plant, with blood levels ~7–16× normal). At Iowa's ambient drinking-water levels it is plausible but unproven and likely small. Calibrated prior that ambient-dose Iowa PFAS meaningfully drives the state's cancer trend: ~2–4%.
What Iowa's water actually contains (I downloaded the EPA data)
I pulled the EPA's UCMR5 monitoring data (152 Iowa public systems) and computed it directly: PFAS is detected in ~21% of systems, and ~9 systems exceed the new 2024 federal limits — but only by 1–9×, in industrial/Mississippi-corridor and firefighting-foam (airport/base) towns, not the 100× of actual source sites.
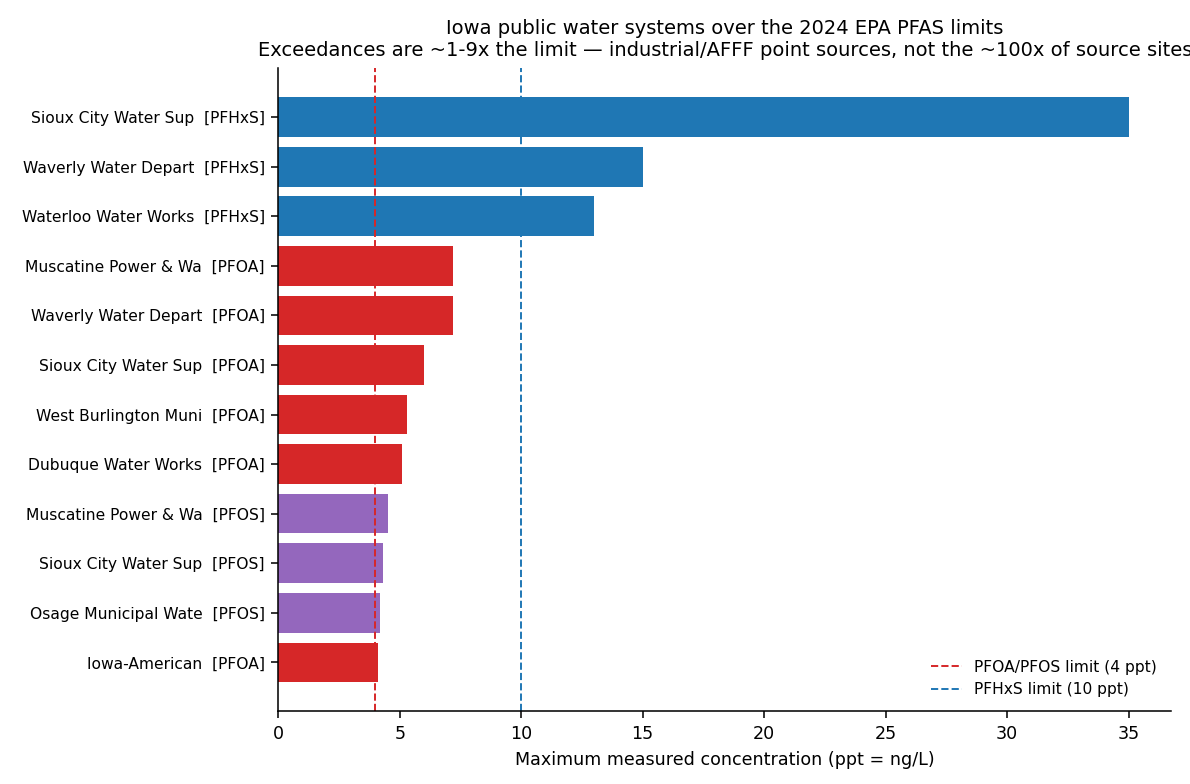
The decisive number: Iowa's dose is below where the cancer signal lives
The cancer studies come from blood levels far above Iowa's. Iowa's 4–10 ppt water translates to blood (serum) levels of only ~2–4 ng/mL — which is the lowest-risk reference group of the very study that found a kidney signal. The kidney dose-response flattens out above ~12.5 ng/mL, and the high-exposure C8 community sat at ~33 ng/mL (you'd need ~190–510 ppt water to get there). On top of that, the headline kidney study failed to replicate in a larger cohort. Iowans on compliant water aren't at the doses where the signal exists.
And Iowa's kidney-cancer rise doesn't implicate PFAS
Iowa is elevated in both PFAS cancers — kidney (20.3 vs 17.8/100k) and testicular (+22% vs US). But Iowa's kidney rise is detection-driven (incidence up, mortality down — incidental CT scans), and elevated testicular rate is partly demographic (it's a young-white-male cancer; Iowa is whiter). Neither pattern, by itself, points to PFAS. The real concern is concentrated at point sources and the ~100,000 untested private wells. Best test: serum-PFAS biomonitoring of those residents linked to the Iowa Cancer Registry — PFAS's advantage is that it's measurable in blood.
The four agents, side by side
| Agent | Strongest evidence | For early-onset GI cancer | Iowa relevance |
|---|---|---|---|
| Nitrate (water) | Human-cancer cohorts (CRC/gastric, HR ~1.16) | Plausible, contested | High — Iowa median in the signal band |
| Emulsifiers (food) | Mechanism (mucus/microbiome); colibactin bridge | Speculative — cohort null for colorectal | Low (no local data) |
| Sweeteners (food) | Microbiome causation (RCT + transplant) | Evidence points the other way; maybe protective | Low |
| PFAS (water, non-microbiome) | IARC Group 1 (PFOA); prospective serum data | Kidney/testicular — but at HIGH dose, not Iowa's | Real but localized (~9 systems); dose too low |
The concrete first step — and it's an Iowa one
Molecular archaeology in the Iowa Cancer Registry
The highest-value, partly confounder-proof study (~$0.3–0.6M): partner with the Iowa Cancer Registry (a gold-standard SEER registry with banked tumor specimens) to whole-genome-sequence ~150 young-onset vs ~150 late-onset Iowa colorectal cancers, look for the colibactin fingerprint, use the molecular "clock" to date when it struck, and link it to each patient's childhood water-nitrate and food environment. If Iowa's early-onset surge carries that early-life fingerprint, you've found a real thread — and a pre-registered null is just as publishable. For nitrate specifically, the decisive design is an individual-level Iowa cohort with measured lifetime residential nitrate (as the Iowa Women's Health Study did) plus biomonitoring.
Hypothesis-generating, unbiased, and honest about uncertainty. Full write-ups:
RESEARCH_PROGRAM_food_water_microbiome.md, NITRATE_IOWA.md,
EMULSIFIERS.md, SWEETENERS.md, PFAS_IOWA.md,
WHY_IOWA_LAGS_AND_EARLY_ONSET.md. Data: analysis/p7_chemical_diet_interaction.py,
p8_nitrate_deep_dive.py, p9_upf_proxy.py, p10_pfas_iowa.py (real EPA UCMR5).
(These are open, falsifiable hypotheses, not conclusions.)